Our immune system, and chronic pain conditions in women
Throughout the world, women are more likely to have a chronic pain condition than men. Why is this happening? And what do we know about the causes of chronic pain?
Chronic pain is pain that persists longer than expected. It is the injury that has healed but pain continues, or the irritable bowel symptoms long after a severe episode of gastroenteritis. In both these situations there was a strong stimulus to the body’s immune system that resulted in changes to the nervous system and a range of different symptoms. So, what is the immune stimulus causing pelvic pain in women?
At Alyra Biotech, we believe that girls and women with severe period pain have excess activation of their immune system in the uterus. And they have it every month for years.
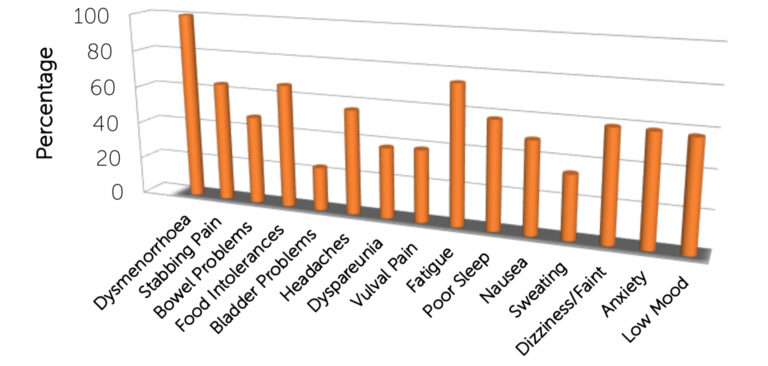
We believe that this puts them at risk of chronic pelvic pain, and a wide range of symptoms both within and outside the pelvis.
And we believe that we can reduce these symptoms by turning down activation of the immune system in the uterus.
Toll-Like Receptor 4, Menstruation and Pain Symptoms in Women
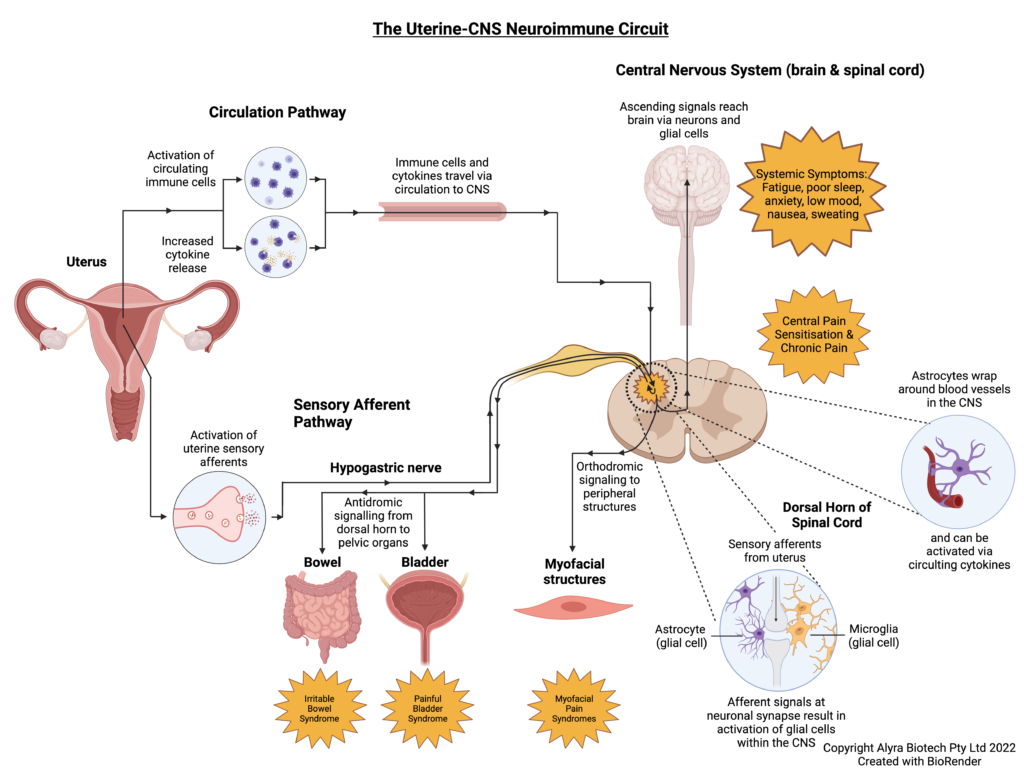
Our immune system has cells that travel around the body looking for bacteria, viruses or damaged tissue that could be a threat to us. Some of these cells (like macrophages) travel through the blood to tissues around the body, and some (called glia) live permanently in the central nervous system. The circulating immune cells bring information from the body to the glia and the glial cells then pass on this information to the nervous system. This system works well for one-off infections or illnesses. However, sometimes repeated activation of the nervous system causes sensitisation, chronic pain and other pain-related symptoms like fatigue, mood changes, or poor sleep. This process involves activation of Toll-Like Receptors (TLR4) on the surface of immune cells.
We already know that this happens in people who develop painful bladder symptoms after recurrent urinary infections, or irritable bowel symptoms in people who have had gastroenteritis. At Alyra Biotech we believe that this also happens in women who have severe period pain every month. We already know that women with endometriosis and pelvic pain have excess activation of TLR4 in their uterus. And we know that cells in the blood of women with pelvic pain react more strongly to stimulation of TLR4 receptors than the cells in the blood of women without pain.
Recurrent episodes of immune-based pain are particularly potent at causing chronic pain.
While it is commonly recognised that bacteria can activate TLR4 receptors, they can also be activated by breaking down tissue, and by blood – all of which are present during menstruation. This makes every painful period another stimulus to a sensitised central nervous system, and an aggravator of chronic pelvic pain symptoms.
Alyra Biotech’s platform approach will provide intrauterine technologies to turn down immune activation in the uterus and protect against this pain. We target the uterus – where immune activation is happening – with tiny amounts of immune inhibiting drug, then use the body’s own immune system to reduce pain. This will minimise the potential for drug side effects or drug-drug interactions.
Alyra Biotech has already completed pre-clinical, cell receptor, human blood and end-user research. In 2024, Alyra Biotech successfully completed a first-in-human trial of our lead device. This cohort will expand with a further 90 participants in 2025.
As with other pain conditions, current treatments are available. However, adverse effects and the need to take these medications daily make them unappealing to young women.
Following preclinical research demonstrating that activation of the immune system in the uterus results in excessive activation of spinal glial cells within the dorsal horn of the spinal cord (a condition seen in chronic pain), Alyra Biotech began development of intrauterine devices that will turn down this activation and thus reduced chronic pain. It is anticipated that these devices will also improve symptoms of an irritable bowel or painful bladder as the nerve supply to all three organs converges on the same segments of the spinal cord: Jobling P. Female Reproductive Tract Pain- targets challenges and outcomes
Our products use intrauterine administration of immune inhibitors to treat bladder and bowel symptoms by reducing spinal glial activation within the dorsal horn.
Medical conditions of the central nervous system that are more common in women
Women are over-represented in populations with conditions of the central nervous system associated with inflammation and activation of the innate immune system. These conditions may present in 3 ways:
- Certain medical conditions affecting the central nervous system are present in both men and women, but are known to be more frequent in females. For example, migraine headache occurs three times as commonly in women than men, affecting approximately 18% of women compared with 6% of men in the United States.
- Certain medical conditions occur only in the luteal phase of the menstrual cycle. For example, Premenstrual Syndrome (PMS) and Premenstrual dysphoric disorder (PMDD) describe a variety of affective, behavioural and somatic symptoms that occur in the luteal phase of the menstrual cycle during a woman’s reproductive years.
- Certain medical conditions may be present throughout the menstrual cycle, but be exacerbated in the days prior to a menstrual period. For example, established psychiatric diagnoses including persistent depressive disorder, major depressive disorder, bipolar disorder and anxiety disorders may be exacerbated premenstrually in a proportion of women.
Where there is an inflammatory component to the medical condition, with activation of circulating immune cells and associated cytokine release, a reduction in immune activation holds promise for effective management.
References
- Bush D, Evans S, Vancaillie T. “The 6 Billion Woman and the $600Million Girl: The Pelvic Pain Report,” 2011. http://www.fpm.anzca.edu.au/Pelvic_Pain_Report_RFS.pdf
- K N Dodds, E A H Beckett, S F Evans, P M Grace, L R Watkins, and M R Hutchinson. “Glial Contributions to Visceral Pain: Implications for Disease Etiology and the Female Predominance of Persistent Pain.” Translational Psychiatry 6, no. 9 (September 13, 2016): e888. https://doi.org/10.1038/tp.2016.168
- Evans, Jemma, and Lois A. Salamonsen. “Inflammation, Leukocytes and Menstruation.” Reviews in Endocrine & Metabolic Disorders 13, no. 4 (December 2012): 277–88. https://doi.org/10.1007/s11154-012-9223-7.
- Evans Sf, Brooks TA, Esterman Aj, Hull Ml, and Rolan Pe. “The Comorbidities of Dysmenorrhea: A Clinical Survey Comparing Symptom Profile in Women with and without Endometriosis.” Journal of Pain Research, 2018, 3181–3194. https://doaj.org/article/d9e23b1430ff4d9386b56d3d2a2f6296.
- Jobling, Phillip, Kate O’Hara, and Susan Hua. “Female Reproductive Tract Pain: Targets, Challenges, and Outcomes.” Frontiers in Pharmacology 5 (2014). https://doi.org/10.3389/fphar.2014.00017.
- Hardi, Gemma, Susan Evans, and Meredith Craigie. “A Possible Link between Dysmenorrhoea and the Development of Chronic Pelvic Pain.” The Australian & New Zealand Journal of Obstetrics & Gynaecology 54, no. 6 (December 2014): 593–96. https://doi.org/10.1111/ajo.12274.
- Khan, K. N., M. Kitajima, K. Hiraki, A. Fujishita, T. Ishimaru, and H. Masuzaki. “Escherichia Coli in Menstrual Blood: An Association with Bacterial Endotoxin and Toll-like Receptor 4 (TLR4)-Mediated Growth of Endometriosis.” Journal of Reproductive Immunology 71, no. 2 (2006): 152–153. https://doi.org/10.1016/j.jri.2006.08.030.
- Khan, Khaleque Newaz, Akira Fujishita, Michio Kitajima, Koichi Hiraki, Masahiro Nakashima, and Hideaki Masuzaki. “Intra-Uterine Microbial Colonization and Occurrence of Endometritis in Women with Endometriosis †.” Human Reproduction 29, no. 11 (2014): 2446–2456. https://doi.org/10.1093/humrep/deu222.
- Kwok, Yuen H., Mark R. Hutchinson, Melanie G. Gentgall, and Paul E. Rolan. “Increased Responsiveness of Peripheral Blood Mononuclear Cells to In Vitro TLR 2, 4 and 7 Ligand Stimulation in Chronic Pain Patients (Increased TLR Responsiveness in Pain Patients)” 7, no. 8 (2012): e44232. https://doi.org/10.1371/journal.pone.0044232.
- Yuen H Kwok, Jonathan Tuke, Lauren L Nicotra, Peter M Grace, Paul E Rolan, and Mark R Hutchinson. “TLR 2 and 4 Responsiveness from Isolated Peripheral Blood Mononuclear Cells from Rats and Humans as Potential Chronic Pain Biomarkers.” PLoS ONE 8, no. 10: e77799. Accessed December 28, 2018. https://doi.org/10.1371/journal.pone.0077799.
- Lacagnina, Michael J., Linda R. Watkins, and Peter M. Grace. “Toll-like Receptors and Their Role in Persistent Pain.” Pharmacology & Therapeutics 184 (April 2018): 145–58. https://doi.org/10.1016/j.pharmthera.2017.10.006
- Erin D. Milligan, and Linda R. Watkins. “Pathological and Protective Roles of Glia in Chronic Pain.” Nature Reviews Neuroscience 10, no. 1 (2009): 23–36. https://doi.org/10.1038/nrn2533.
- Nicotra, Lauren, Lisa C. Loram, Linda R. Watkins, and Mark R. Hutchinson. “Toll-like Receptors in Chronic Pain.” Experimental Neurology 234, no. 2 (2012): 316–329. https://doi.org/10.1016/j.expneurol.2011.09.038.
- Lauren Nicotra, Jonathan Tuke, Peter Grace, Paul Edward Rolan, and Mark Rowland Hutchinson. “Sex Differences in Mechanical Allodynia: How Can It Be Preclinically Quantified and Analysed?” Frontiers in Behavioral Neuroscience 8 (2014): 40. https://doi.org/10.3389/fnbeh.2014.00040.
- Perquin, Christel W, Alice A. J. M Hazebroek-Kampschreur, Joke A. M Hunfeld, Arthur M Bohnen, Lisette W. A van Suijlekom-Smit, Jan Passchier, and Johannes C van der Wouden. “Pain in Children and Adolescents: A Common Experience.” Pain 87, no. 1 (July 1, 2000): 51–58. https://doi.org/10.1016/S0304-3959(00)00269-4.
- Watkins, Linda R., Erin D. Milligan, and Steven F. Maier. “Glial Activation: A Driving Force for Pathological Pain.” Trends in Neurosciences 24, no. 8 (August 2001): 450–55. https://doi.org/10.1016/S0166-2236(00)01854-3.